上海复旦胸外团队发表最新食管癌临床研究:三野淋巴结清扫对比二野淋巴结清扫
点击:865次时间:2020-03-09 10:11:33
关于食管癌淋巴结清扫的最佳范围一直存在争议。淋巴结扩大清扫的优点是可以清除所有潜在的肿瘤累及的淋巴结,以提供准确的肿瘤分期。但淋巴结扩大淋巴结清扫是否能给患者带来生存效益尚不确切,并可能导致更高的手术并发症发生率。
之前有食管鳞癌的随机试验显示,经右胸入路扩大的二野淋巴结清扫与经左胸入路较小范围的胸腹二野淋巴结清扫相比没有增加手术风险,但淋巴结阳性的患者可能受益于扩大的淋巴结清扫,减少局部区域复发,提高整体生存率。
而食管癌颈部淋巴结转移的发生率很高,因此,三野淋巴结清扫对于可能存在颈胸腹淋巴结转移的患者来说很有必要,但二野和三野淋巴结清扫的利弊如何,目前针对中国人群的研究并不多。
近日,上海复旦胸外科陈海泉教授团队领衔的一项单中心随机对照临床研究在线发表在国际知名外科杂志《British Journal of Surgery》上。
一项随机临床试验:食管鳞癌经胸食管切除术二野淋巴结清扫与三野淋巴结清扫的近期结果比较
— 结论 —
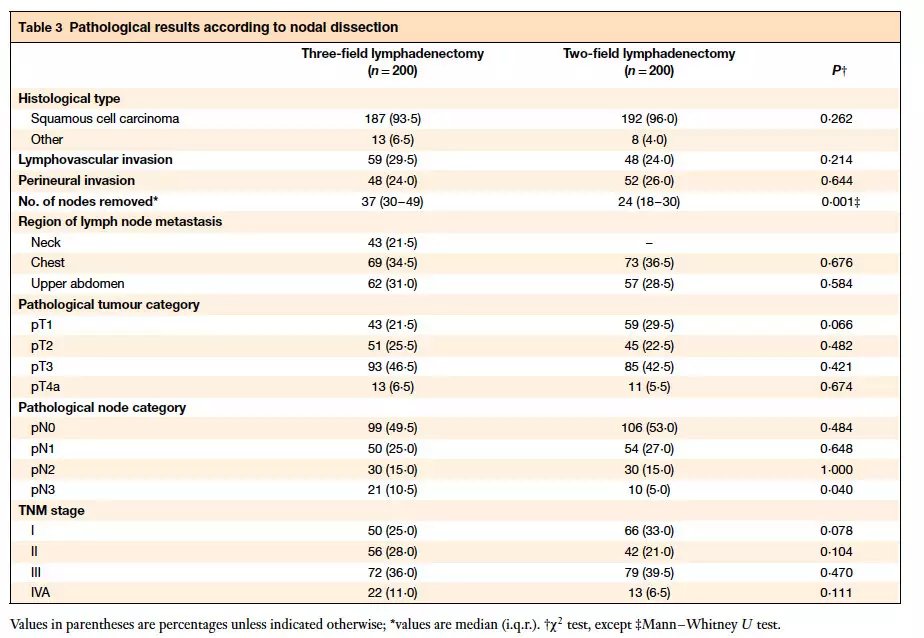
食管切除加三野淋巴结清扫增加了淋巴结的切除数目,并且由于颈部淋巴结转移率高达21.5%而导致术后病理分期增加。两野和三野淋巴结清扫术的术后并发症大体相当。
Oesophagectomy with three‐field lymphadenectomy increased the number of lymph nodes dissected and led to stage migration owing to a 21·5 percent rate of cervical lymph node metastasis. Postoperative complications were largely comparable between two‐and three‐field lymphadenectomy.
— 目的 —
食管癌三野淋巴结清扫的利弊尚不明确。本研究的目的是比较食管鳞癌患者三野和二野淋巴结清扫的总生存率、并发症发生率和死亡率。
The benefit and harm of three‐field lymphadenectomy for oesophageal cancer are still unknown. The aim of this study was to compare overall survival and morbidity and mortality between three‐and two‐field lymphadenectomy in patients with oesophageal squamous cell carcinoma.
— 方法 —
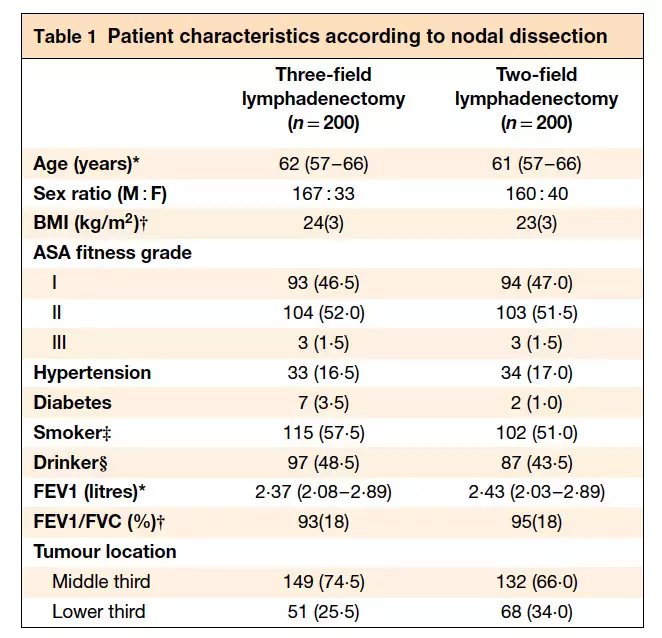
2013年3月至2016年11月,纳入胸中段、下段食管鳞癌患者,被随机分配到开放性食管切除术+三野(颈胸腹)或二野(胸腹)淋巴结清扫组。患者术前未接受(放)化疗。
本次报告的为本研究的次要研究结果:病理学结果和外科并发症发生情况(该临床研究的主要研究终点为总生存率)。
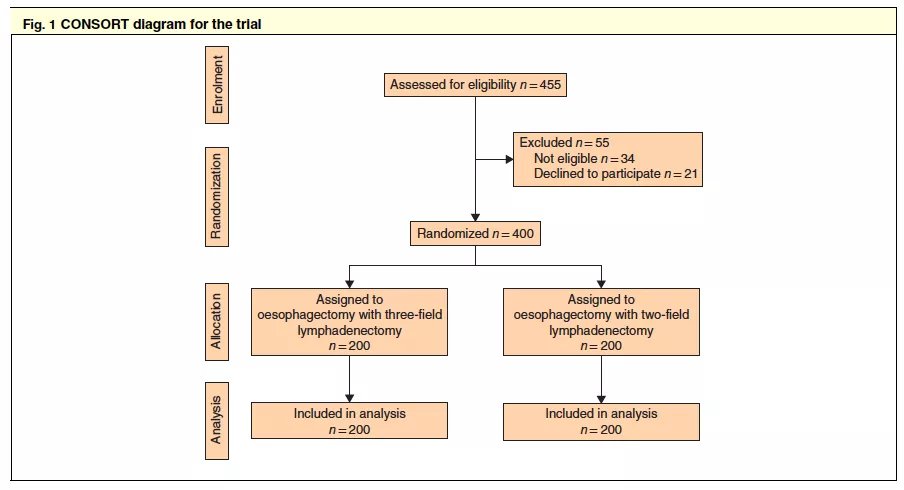
Between March 2013 and November 2016, patients with squamous cell carcinoma of the middle or distal oesophagus were assigned randomly to open oesophagectomy with three‐field (cervical–thoracic–abdominal) or two‐field (thoracic–abdominal) lymphadenectomy. No chemo(radio) therapy was given before surgery. This paper reports on the secondary outcomes of the study: pathology and surgical complications.
—结果—
400名患者被随机分配至两组,每组200名。
三野清扫组的平均淋巴结切除率为37个(四分位区间:30–49),而二野清扫组为24个(18–30)(P<0.001)。三野清扫组中,43例(21.5%)有颈部淋巴结转移。
三野清扫组有更多的pN3期患者:三野清扫组21例(10.5%),二野清扫组10例(5.0%)(P=0.040)。
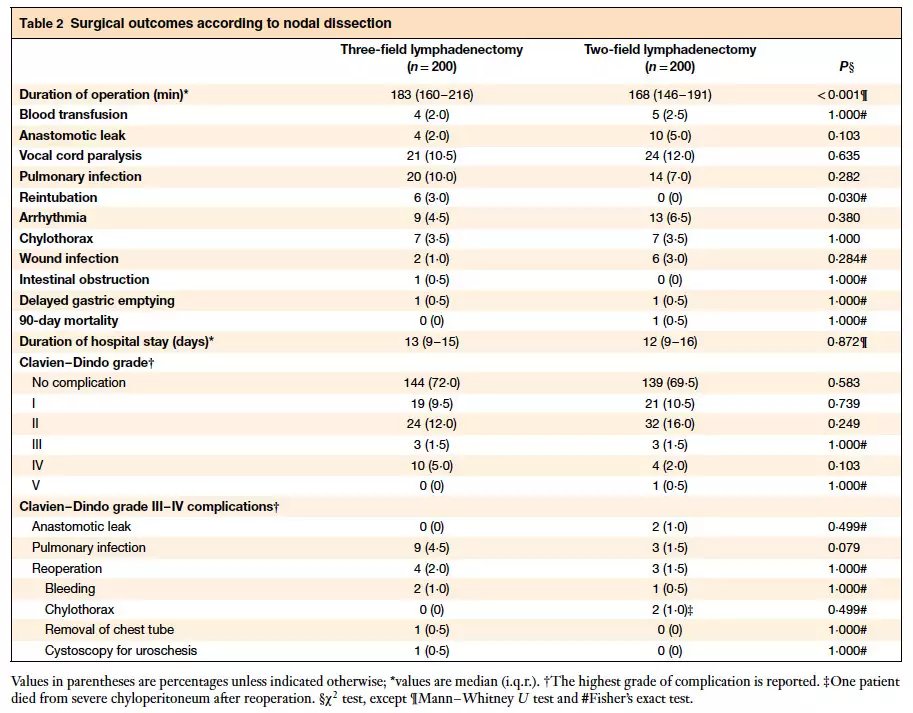
两组术后并发症的发生率和严重程度差不多,但三野清扫组有6例需要重新插管,而两野清扫组没有(3.0对0%;P=0.030)。
三野清扫组90天死亡率为0%,二野清扫组为0.5%(1例)(P=1.000)。
Some 400 patients were randomized, 200 in each group. A median of 37 (i.q.r. 30–49) lymph nodes were dissected in the three‐field group, compared with 24 (18–30) in the two‐field group (P < 0·001). Some 43 of 200 patients (21·5 per cent) in the three‐field group had cervical lymph node metastasis. More patients in the three‐field group had pN3 disease: 21 of 200 (10·5 per cent) versus 10 of 200 (5·0 per cent) (P = 0·040). The rate and severity of postoperative complications were comparable between the two groups, except that six patients in the three‐field arm needed reintubation compared with none in the two‐field group (3·0 versus 0 per cent; P = 0·030). The 90‐day mortality rate was 0 per cent in the three‐field group and 0·5 per cent (1 patient) in the two‐field group (P = 1·000).
—附图—
|
Copyright © http://www.cstcvs.net 2000-2026 all Reserved. 京ICP备16013221号-1 |
 胸心分会官方公众号 |